If your medical device depends on Google Cloud, your cloud setup is part of the device. That means GCP security affects patient safety, HIPAA scope, and FDA review at the same time.
I’d boil this guide down to four points:
- Map the full system, not just the device: include apps, APIs, update paths, cloud storage, admin access, and audit records.
- Separate data, control, and evidence paths so PHI, device commands, and audit artifacts don’t get mixed together.
- Tie each risk to a control: least-privilege IAM, private networking, CMEK, audit logs, Terraform, Binary Authorization, and SBOM tracking.
- Keep proof ready: architecture diagrams, IAM records, logs, threat models, signed builds, and vendor reports should all support HIPAA and FDA checks.
One fact sets the tone here: the 2024 Change Healthcare breach affected more than 192 million people. For U.S. healthcare teams, that’s a reminder that cloud-connected device systems can fail at scale.
I’d use this guide to answer three direct questions:
-
What is in scope?
The device, companion software, GCP services, update systems, identities, keys, and clinical data paths. -
What controls matter most?
Strong identity rules, encrypted data paths, private access to PHI stores, version-controlled infrastructure, and tamper-evident logging. -
What will auditors ask for?
Clear risk files, SBOMs, change records, access logs, and proof that each cloud service was reviewed and set up with intent.
A few points stand out right away:
- FDA Section 524B applies to connected “cyber devices,” including ones with dormant network interfaces.
- As of 02/02/2026, the FDA’s QMSR aligns 21 CFR Part 820 with ISO 13485:2016, which puts more weight on supplier control and risk-based change review.
- If PHI is involved, you need a BAA with Google, and only covered products should handle that data.
- PHI should never go into metadata, labels, titles, or metrics, because those fields can show up in places many people can read.
Here’s the short version of the security model I’d keep in mind:
| Area | What to focus on |
|---|---|
| Scope | Device-to-cloud data flows, trust boundaries, critical assets |
| Risk review | STRIDE threats, patient-harm impact, third-party risk management |
| Core controls | IAM, mTLS, private IP, CMEK, logging, IaC, image approval |
| Audit proof | SBOMs, access logs, diagrams, threat models, build attestations |
So if you want the plain answer: secure the cloud like it is part of the device, document it like an auditor will inspect it, and review every change like it could affect care.
GCP Assured Workloads for HIPAA: A Beginner's Guide to Cloud Compliance
sbb-itb-535baee
GCP Basics for Medical Device Security
Before you can design controls that matter, you need a clear view of how GCP fits into a medical device setup.
Medical Device Architectures on GCP
Once scope is set, map the device's GCP touchpoints.
Google Cloud can support regulated medical software, but that only works when device controls, data handling, and access rules are planned as one system.
In most connected device setups, GCP shows up in three main places: ingest, storage, and access. Telemetry and images can flow in through Cloud Healthcare API and Pub/Sub. Data can then live in Cloud Storage, Cloud SQL, Spanner, or Bigtable. Analytics may run in BigQuery or Vertex AI, and dashboards can be exposed through Looker and IAP [3][4].
Data at rest is often protected with CMEK, which lets the manufacturer keep control over decryption [3][4]. Modern software as a medical device (SaMD) also leans on cloud services to coordinate firmware and mobile apps [3].
That mix matters. PHI, operational telemetry, and safety-critical functions often sit in the same environment. If you don't map each one to the right storage location and access rule, things get messy fast.
U.S. Regulatory Requirements and Security Frameworks
The FDA's QMSR (21 CFR Part 820) alignment with ISO 13485:2016 in early 2026 makes GCP configuration part of risk-based change control and outsourcing decisions [3].
If PHI is involved, you need to execute a BAA with Google and make sure only Covered Products under that agreement handle PHI [4][6]. That's not a small paperwork step. It shapes what can be used, where PHI can go, and who is on the hook for each control.
These rules also draw a hard line between Google's role and yours.
Shared Responsibility on GCP
Google secures the platform. You secure configuration, access, applications, and device-layer controls.
| Area | Google's Responsibility | Your Responsibility |
|---|---|---|
| Physical security | Data center access, environmental controls | N/A |
| Infrastructure | Hardware, network paths, patching | VM configuration, application architecture |
| Data protection | Default encryption at rest/transit | Key management (CMEK), data classification |
| Access control | IAM platform availability | Least-privilege roles |
| Compliance evidence | Platform certifications (ISO, SOC, HITRUST) | SBOM generation, audit trail configuration |
One rule is easy to miss: never place PHI in metadata, labels, or dashboard titles. Those fields can appear in logs and views that have broad read access [4].
Those boundaries set the scope for the risk assessment that follows. Effective cyber risk management ensures these boundaries protect both data and patient safety.
Risk Assessment for Device-to-GCP Workloads
GCP Security Controls for Medical Devices: STRIDE Threat Model & Controls
Use the shared-responsibility split to define the full device-to-cloud risk boundary.
Define Scope, Data Flows, and Critical Assets
Stopping at the physical device is a regulatory gap. You need to scope the full system around it: companion apps, backend services, update servers, and the clinical setting where the device is meant to operate.
Under FDA Section 524B, a "cyber device" includes any device with software that can connect to the internet, even through dormant interfaces[7]. That means the boundary is broader than many teams first assume. Build DFDs that show every entry point, trust boundary, and device-to-cloud data path[7]. Then classify PHI, telemetry, configs, keys, and update packages as separate asset types[7].
A simple way to structure GCP workloads is to split them into three planes:
- The Data Plane handles clinical and device data with CMEK
- The Control Plane manages identity and network access with Zero Trust and IAP
- The Evidence Plane stores audit trails, build attestations, and SBOMs[3]
Once scope and assets are clear, the next step is to tie each trust boundary to a threat.
Threat Modeling and Control Mapping
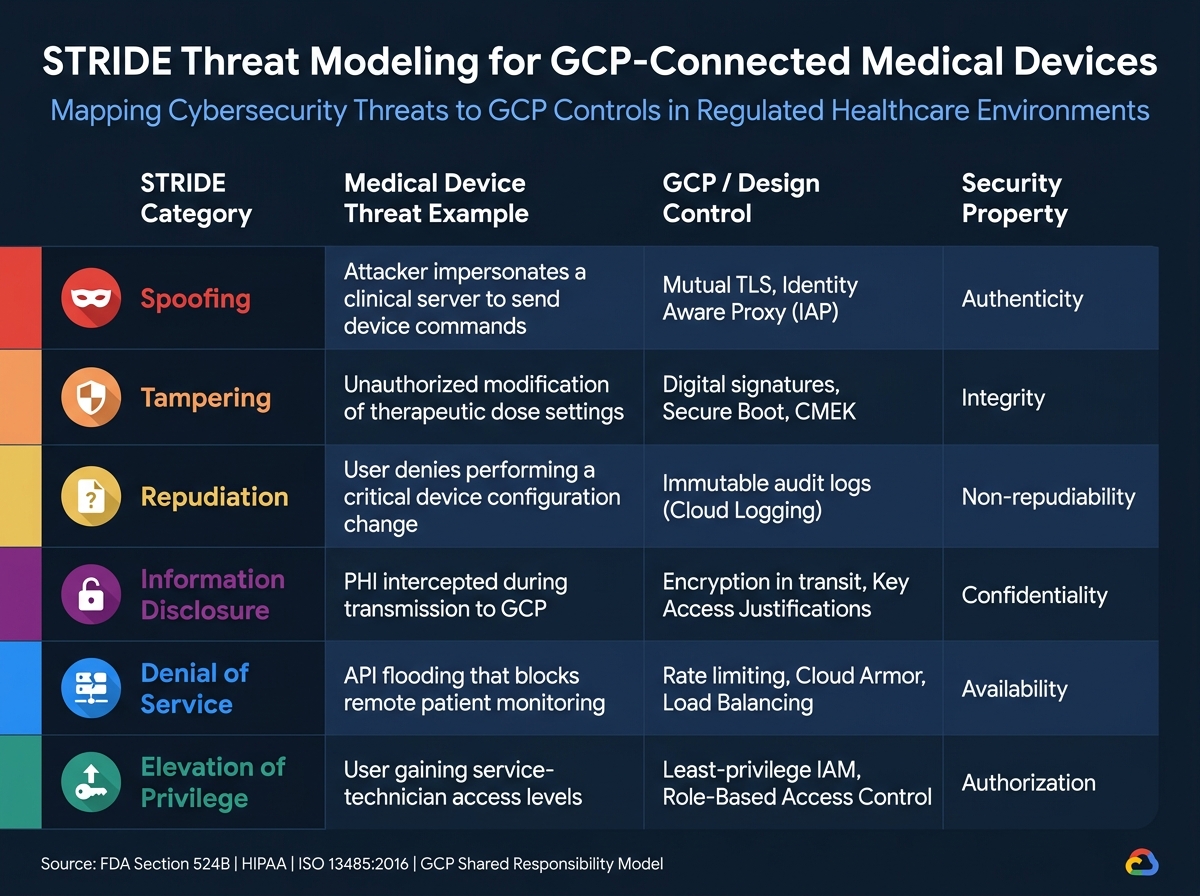
With assets and data flows documented, apply STRIDE to every DFD element. STRIDE stands for Spoofing, Tampering, Repudiation, Information Disclosure, Denial of Service, and Elevation of Privilege[7]. The table below connects each category to a medical device threat and the GCP or design control used to address it.
| STRIDE Category | Security Property | Example Medical Device Threat | GCP / Design Control |
|---|---|---|---|
| Spoofing | Authenticity | Attacker impersonates a clinical server to send device commands | Mutual TLS, Identity Aware Proxy (IAP) |
| Tampering | Integrity | Unauthorized modification of therapeutic dose settings | Digital signatures, Secure Boot, CMEK |
| Repudiation | Non-repudiability | User denies performing a critical device configuration change | Immutable audit logs (Cloud Logging) |
| Information Disclosure | Confidentiality | PHI intercepted during transmission to GCP | Encryption in transit, Key Access Justifications |
| Denial of Service | Availability | API flooding that blocks remote patient monitoring | Rate limiting, Cloud Armor, Load Balancing |
| Elevation of Privilege | Authorization | User gaining service-technician access levels | Least-privilege IAM, Role-Based Access Control |
After that, rank each mapped risk by likelihood and patient impact. If a threat could interrupt care or lead to direct patient harm, it should move to the top of the queue even if the attack path looks hard to pull off.
Risk Prioritization and Third-Party Assessment
Once threats are mapped to controls, rank them by exploitability and patient-harm severity[7]. In practice, this keeps the team focused on what matters most. A low-frequency issue that could disrupt therapy may deserve more attention than a simpler bug with little clinical effect.
Treat GCP services and dependencies as SOUP: document each service's requirements, dependencies, and risk[2]. Also pin service tiers, runtimes, and images so unvalidated provider updates don't change validated device behavior[2]. That's one of those details that sounds small until it isn't.
Google Cloud's compliance reports, including SOC 2/3, ISO/IEC, and HIPAA materials, can serve as base evidence for vendor assessments and cut down the amount of one-off qualification work[1]. Use that foundation to focus effort on the items with the highest risk first.
| Risk Treatment Approach | Healthcare Use Case | Risk Reduction | Operational Burden | Audit Implications |
|---|---|---|---|---|
| Infrastructure-as-Code (IaC) | Cloud misconfiguration | High; reproducible, version-controlled environments | Moderate; requires DevOps expertise | Supports EN 62304 configuration management |
| Version Pinning | Insecure / unvalidated updates | High; prevents unvalidated provider changes | Low; requires strict config policies | Critical for maintaining a validated frozen state |
| Multi-AZ Redundancy | Operational downtime | High; protects against regional outages | Moderate; increases GCP costs | Supports availability requirements in safety risk files |
| Least-Privilege IAM | Credential theft | High; limits blast radius of compromised accounts | Moderate; requires ongoing permission audits | Directly addresses FDA and HIPAA access control requirements |
| SBOM Monitoring | Vendor-related exposure | High; surfaces vulnerabilities in SOUP components | High; requires continuous scanning | Mandatory for FDA Section 524B compliance |
Update the risk file whenever the SBOM or design changes[7]. If a new vulnerability shows up in a third-party component listed in the SBOM, reassessment starts right away[7]. Treat a stale SBOM as missing[7].
GCP Security Controls for Medical Device Data and Operations
You’ve finished the risk assessment and mapped threats to controls. Now comes the part that matters in day-to-day operations: putting those controls into production.
Apply them across the data, control, and evidence planes identified earlier. In plain terms, this section turns risk analysis into actual GCP setup choices across three areas: identity and keys, network and storage, and logging and change control. As you go, tie each control back to the risk and asset it protects.
Identity, Device Authentication, and Key Management
Start with least-privilege IAM for service accounts and device credentials. Give each identity only the access it needs. No more. No less.
Use short-lived credentials whenever you can, and avoid long-lived service account keys. Long-lived keys tend to stick around, get copied, and become a problem later.
For PHI storage and other high-sensitivity repositories, review whether Customer-Managed Encryption Keys (CMEK) make sense, even though GCP encrypts data at rest by default [4].
| Feature | Google-Managed Keys | Customer-Managed Keys (CMEK) |
|---|---|---|
| Control Level | Google manages lifecycle and rotation | Customer controls key rotation and access policies |
| Operational Complexity | Low (default setting) | Moderate (requires Cloud KMS management) |
| Typical Healthcare Use Case | Standard PHI protection for general workloads | High-sensitivity data requiring strict sovereignty or contractual control |
For high-sensitivity workloads, CMEK paired with Key Access Justifications (KAJ) gives you traceability for key use [3][5]. That matters when you need to show who accessed what and why.
One more rule here: do not place PHI in metadata, labels, titles, or metrics.
Once identity and key controls are in place, move to the data path and storage layer.
Network Segmentation, Secure Data Paths, and Storage Protections
Separate workload tiers with VPC design and firewall rules built around explicit allow-lists. That keeps traffic paths tight and cuts down exposure.
Use Private IP connectivity for services such as Cloud SQL and Database Migration Service so databases that contain PHI are never reachable from the public internet [4]. That’s a simple line of defense, but it goes a long way.
On the storage side, turn on Object Versioning in Cloud Storage for every bucket that stores clinical data or device telemetry. If someone deletes an object by mistake, you have a path to recovery without adding extra tools. Pair that with Cloud SQL point-in-time recovery and Filestore backups to cover the full data layer [4][5].
A few storage guardrails matter here:
- Restrict storage access with IP allow-lists where that fits your architecture.
- Use only BAA-covered products for PHI workloads [4].
Logging, Monitoring, Patching, and Change Control
Enable both Admin Activity and Data Access audit logs. Then export them to Cloud Storage for long-term archival and to BigQuery for search, investigation, and forensic work [4].
These logs are your audit evidence. They should capture device commands, firmware updates, and admin actions. Use immutable logs so audit records are tamper-evident.
Security Command Center (SCC) and Cloud Monitoring help spot unencrypted buckets, open firewall rules, and policy drift before they turn into audit findings. Route SCC alerts into CAPA or deviation workflows [5]. That way, alerts don’t just sit there. They feed action.
Patching needs clear ownership. Google patches hypervisors and hardware. You patch Compute Engine VMs, GKE node pools, and other customer-managed parts. That split matters, especially in regulated setups where people often assume the cloud provider handles more than it does.
Use Infrastructure as Code (IaC) with Terraform so each configuration change is version-controlled and auditable [5]. Think of every infrastructure change as part of the device’s validated state. Terraform history then becomes change-control evidence, and Binary Authorization can block unapproved production images [3].
These records feed the audit and governance work that follows.
Compliance, Audit Readiness, and Ongoing Governance
These controls should do more than protect systems. They should leave behind an audit trail that regulators can check line by line. From there, the job is to turn those controls into an audit package and a standing governance process.
Demonstrating HIPAA and FDA Alignment
Use the controls above as evidence, not just safeguards.
For HIPAA, keep audit logs, IAM records, CMEK policy settings, and key-access records in a format that links each event to a specific asset and data flow.
FDA reviews cybersecurity as part of QMSR-based device oversight, and weak records can create misbranding exposure under the FD&C Act. Vulnerability scanning built into CI/CD helps support FDA postmarket cybersecurity expectations.
Treat compliance like code: write controls into policy, collect the artifacts they create, and keep those artifacts ready for review.
Evidence Collection and Audit Preparation
Group evidence by the control it proves.
Include architecture diagrams, data-flow maps, IaC, IAM roles, access logs, SBOMs, signed build attestations, threat models, and scan results. Document each GCP service’s functional and performance requirements, along with its risk impact. Add Google’s SOC 2/3 reports and HIPAA attestations as supporting evidence.
| Evidence Category | Specific Records | GCP Tooling |
|---|---|---|
| Architecture | Data flow maps, network diagrams, trust boundaries | Cloud Architecture Center, IAP |
| Configurations | IaC files, Organization Policy logs | Terraform, Org Policy Service |
| Identity/Access | IAM roles, Data Access Logs, Key Access Justifications | Cloud IAM, Cloud Logging |
| Supply Chain | SBOM, signed build attestations | Artifact Registry, Binary Authorization |
| Risk/Threats | Threat models, vulnerability scan results, pen test reports | Security Command Center |
Continuous Risk Management for GCP-Connected Devices
Audit readiness falls apart if change control slips.
Governance needs to run all the time: scan for vulnerabilities, review logs on a set cadence, and trigger impact checks before Google or device updates hit production. Give each governance task a clear owner across the data, control, and evidence planes. For AI-enabled devices, Vertex AI Model Monitoring tracks model drift on a continuous basis - when performance moves away from the validation baseline, it should automatically trigger a CAPA process[1].
The manufacturer - not the hyperscaler - owns the regulatory duty. Google provides the infrastructure. Your team sets it up, watches it, and answers for it.
FAQs
How do I define what’s in scope on GCP?
Map the full technical footprint of each medical device on Google Cloud. That means the whole stack: hardware interfaces, wireless protocols, software layers, APIs, and every cloud dependency tied to the device.
If a cloud service touches the device, or device data crosses any boundary, it belongs in scope.
Use data-flow and architecture diagrams to make those boundaries clear. Then review:
- Connectivity
- Exposure
- Criticality
This helps you understand inherent risk and check that the system supports its intended use.
Put simply: if the device talks to it, depends on it, or sends data through it, document it.
When should a medical device team use CMEK?
Use CMEK when your team needs direct control over data decryption, must meet specific requirements such as HIPAA or GDPR, or needs to manage the full encryption key lifecycle.
It also makes sense when you need to choose key location, set rotation policies, log key access, or use crypto-shredding after a security event. If not, Google-managed default encryption may be enough.
What audit evidence should we keep ready?
Keep documentation in one place, organized around the FDA’s 11 eSTAR cybersecurity categories. That includes a cybersecurity risk management report linked to patient safety and a machine-readable SBOM that covers proprietary, third-party, and open-source components.
You’ll also want to keep design and architecture records, testing evidence, and post-market documentation together with it. The key is clear traceability: each identified threat should map to the control used to address it and the test case used to verify it.
